|
|
Pediatric Occupational, Physical, ABA/Behavioral, Feeding, Speech, and Language Therapies Main Clinic: 931-372-2567 1445 East 10th Street Cookeville, TN 38501 Email: [email protected] HIPAA Secure Email: [email protected] Fax: (931) 372-2572 ABA Clinic: 931-201-9534 400 Dubois Road Cookeville, TN 38501 Email: [email protected] Please call today to get started! Most insurances accepted! |

|
| Who needs therapy? | SE HABLA ESPAÑOL |
|
Home
> Vision is more than seeing 20/20
Vision is more than seeing 20/20 |
|
Related Topics: |
Ready for School…but ready to learn?
As another school year rolls around I often wonder how many children come to school ready to learn?
Most children are up to date on new school clothes, new backpacks, school supplies, and physical check-ups.
Many do not have one the most essential needs covered…a comprehensive eye examination from an eye doctor.
This is one of the most important “to-dos” and yet one that is often overlooked. In many states it is the law that a child have a vision exam with an eye doctor before registering for school. Many children have vision problems that remain un-diagnosed, and often misdiagnosed as a learning disorder, ADHD, avoidance of near work or even behavior problems.
The idea that children need to be ready to learn—visually—is beginning to catch the attention of legislators.
Kentucky, Missouri, and Illinois have laws requiring mandatory eye examinations from a licensed eye doctor (not Lion's Club, pediatric or school screening) for children prior to entering school, and a federal bill has been introduced in the Senate.
So what’s so important about having a comprehensive vision exam with an eye doctor? Why are vision screenings not enough?
Consider that 80% of what your child’s brain processes comes through their primary sense…vision.
Vision is a lot more than seeing 20/20.
For example, vision involves eye muscles working together and holding a focus at near, like a fine motor task. Children with low muscle tone often have Convergence Insufficiency (CI).
CI is a condition where the visual muscles fatigue easily when focusing at near for reading, school work, or doing homework. If a child has difficulty holding a pencil with the appropriate tripod grasp and open web space...or has difficulty doing buttons or tying their shoes...or slumps at their desk, then they often have difficulty with the fine muscle control required to converge their eye muscles to focus at near for very long periods of time in the classroom.
Over 57% of school-age children have a vision disorder, many go undiagnosed because they have never had a comprehensive vision exam from an eye doctor. There are many visual conditions missed by screenings.
While vision screenings can uncover some severe vision problems, they can miss many. This is a major concern about vision screening programs.
They can create a false sense of security for those individuals who "pass" the screening, but who actually have a vision problem, thereby delaying further examination and treatment.
While well intentioned, these individuals do not have the knowledge of an EYE DOCTOR who spends 4-8 years studying vision.
There is often a misunderstanding about what passing a vision screening means. The information obtained from a vision screening can be compared to the information obtained from a blood pressure measurement. Because your blood pressure may be in normal range, it cannot indicate that you do not have other health problems. It provides a single measure of one aspect of your overall health. Just like a complete physical is needed to evaluate total health, only a comprehensive eye and vision examination can evaluate your overall eye health and vision status.
A comprehensive vision examination can only be conducted by an optometrist or ophthalmologist, who has the specialized training needed to make a definitive diagnosis and prescribe treatment. If your child has a learning disorder or special needs, make sure to see an eye doctor who has a fellowship in vision development (F.C.O.V.D. behind their doctorate name).
Frequency of Comprehensive Vision Examination by Eye Doctor
| - - - - - - Examination Interval - - - - - - | ||
| Patient Age | Asymptomatic/Risk-Free | At Risk |
| Birth to 24 Months | At 6 months of age | At 6 months of age or as recommended |
| 2 to 5 years | At 3 years of age | At 3 years of age or as recommended |
| 6 to 18 years | Before first grade and every two years thereafter | Annually or as recommended |
| 18 to 60 years | Every two years | Every one to two years or as recommended |
| 61 and older | Annually | Annually or as recommended |
To learn more please visit www.drclopton.com, www.covd.org, & www.aoa.org
How can OT & VT help Dyslexia, ADHD, Visual issues & Learning?
Occupational therapy for visual dysfunction, impairments, reading delays vs. Vision Therapy
Visual dysfunction is often overlooked during a vision screening at school or the pediatrician’s office.
There are over 20 different areas to evaluate that involve vision, visual attention, visual motor, visual perceptual skills, and lots of more that are shared by the eye doctor and OT.
For best treatment of any delays in reading, attention, focus, avoidant behaviors of sitting and focusing or for any eye disorders like Convergence Insufficiency or Strabismus (eye turns) you would want the following for your child:
- COMPREHENSIVE VISION EXAM by an eye doctor that has obtained a Fellowship from the College of Vision and Development (COVD.org) ASAP.
Do NOT rely on a screening, school exam, or pediatrician’s exam these do not look at all 20 + areas that affect your child’s learning, attention and vision. - Ask your COVD
 DR about Home treatment plan or in office vision therapy if available.
DR about Home treatment plan or in office vision therapy if available.
Follow the eye doctor’s home program for the visual issues daily and purchase Piggyback and all treatments for home, set up consultations with the COVD eye doctor regularly. - Get the right kind of comprehensive Pediatric OT evaluation that includes the following & treatment with OT for these delays- don’t be afraid to ask the OT if they cover this in their testing, this is a specialized area of pediatric OT & and usually includes a OT that collaborates and works with a COVD fellowship trained eye doctor.
OT eval should include:
- Reflex Testing- there are many reflexes that if not integrated can cause vision, learning, attention and focus issues.
- Praxis testing- OT can do a full evaluation of motor coordination and determine if Dyspraxia is causing reading and writing delays. We use the full standardized BOT-3 for this.
- Laterality and Directionality testing- if your child does not know the difference between right and left on them selves and on others they are looking at and/or are having issues with knowing the differences in b,d,p,q or having reversals past the normal age of-6-7 then reading is very difficult and writing due to delays in this area.
- Dominance testing- if a child has mixed dominance then this can cause delays in reading, writing, and letter recognition.
- Vestibular testing that includes eyes closed vs. eyes open, nystagmus testing and vestibular -visual processing and integration. The vestibular system GREATLY affects the visual system and delays in vestibular processing can cause issues with convergence and divergence, visual tracking left to right to read and write, visual attention in central focus and near focus, eye turns, and attention issues.
- Muscle tone- a child with lower or higher muscle tone can have issues with their visual system and this can affect their ability to smoothly visually track and focus at near and then at far.
Convergence insufficiency for example is an issue of vestibular processing and muscle tone and can be treated with OT based exercises working with your COVD eye doctor.
- Visual Motor, Visual Perceptual & Fine Motor Coordination testing- all of these individual areas are treated by OT and can greatly affect a child’s ability to read and write if delayed.
What are these terms and how do they effect reading or look like Dyslexia?
Visual Perceptual Skills- Visual perception is the ability of our brains to interpret that information.
In the most basic sense, it’s the translation piece of the puzzle.
Visual perceptual skills include several skills that describe how our world around works:
 Visual Figure-Ground- Figure ground refers to the visual perception ability to distinguish details of the foreground from the background. The eye is capable of discerning details within a busy field of perception in order to focus on a specific object or part.
Visual Figure-Ground- Figure ground refers to the visual perception ability to distinguish details of the foreground from the background. The eye is capable of discerning details within a busy field of perception in order to focus on a specific object or part.- Visual Closure- Visual closure is the ability of the eyes to visualize a complete image or object when on only a portion is seen. We can recognize just part of a letter or number and know how to visually complete that character without thinking through each line. We can read a sentence without taking the time and effort to focus on each letter and how it is made.
- Visual Spatial Relations- This area of visual perception is the awareness or inattention that impacts the awareness of the body and environment in relation to other objects, forms, or areas. This can present in relationship to others when moving in the classroom or other environment, or can present in handwriting with the placement of the letters. This perception includes directional language concepts as well as movement-based actions. Spatial perceptions can be further broken down in to position in space, depth perception, and topographical orientation.
- Visual Attention- This visual skill is part of the eye’s ability to collect visual information, and is essential for obtaining visual input through the eyes for object recognition and identification.
Visual attention is a voluntary motor skill set of eye movements including visual fixation, gaze shift, ocular pursuit, and localization.
Visual attention and its components are needed for active learning, selective attention, or filtering of information, detection of information happening in the peripheral and immediate fields of vision, as well as shared visual attention.
Many of our kids who struggle with learning and visual fixation are demonstrating challenges with visual attention. Is this a difficulty that results from screen use and that eye shift and scanning that occurs when watching screens!
The lack of focusing at far in play such as outdoor play ( running & play in open spaces and playing in the woods ) is causing more and more of these visual attention delays & issues.
- Visual Memory- This visual perception skill involves the storing of visual information according to aspects of the object or item that is seen. This receptive component of visual processing involves the intake of aspects of objects including characteristics such as size, shape, color, and other details.
The lack of play with manipulative, objects, and more screen time is taking away the development of this.
Visual memory then includes integration of visual information with the “mind’s eye” in regards to previous experiences. Visual memory is necessary for copying work, spelling words, sight words, math facts, sequencing, sorting, and recalling visual information such as names, numbers, and other written work.
- Visual Discrimination- This is a receptive visual perceptual skill that involves discernment of features of an object, including parts, or whole aspects and specific details or general features. Discrimination allows us to match items and categorize similarities and differences in visual information.
- Form Constancy- This visual perceptual skill is the ability to recognize similarities between two forms that are alike or the same, no matter their position, font, direction, size, or other feature. Form constancy allows us to recognize upper- and lower-case letters as the same letter, sight words when positioned in text, and differences between similar letters or words.
- Visual Sequential Memory- This visual perception skill is the ability to sequence visual information, such as in patterning and in remembering information in an order.
- Visual Motor Integration- Visual motor is the integration of the visual information and the motor skills that we perform to complete actions based on that visual information.
This skill area is often times called eye-hand coordination, however, it’s a bit more than that. Visual motor skills are needed to copy use the visual information as it is processed and use it complete motor tasks.
Eye-hand coordination refers to the use of the hands together with information received from the eyes to catch a ball, use tongs, thread beads, etc.
Skills such as handwriting, copying block forms, cutting on lines, coloring in lines, copying tangram forms, etc. are beneficial to working on visual motor skills.
- Sequencing, vision & language - these activities develop the ability to order and remember tasks, or information, correctly. Sequencing involves relating one thing to another - when we read we need to relate words to one another, in the correct order, to obtain meaning from the words.
Sequencing is essential for sounding out words, for comprehension when reading, for spelling and for remembering instructions.
- Visual thinking - these activities develop organized high level visual thinking, especially visual memory and visualization. Simple codes are used initially, then visual matching is developed, followed by visual memory and visual transposition. In this section visual information is usually flashed very quickly, at 0.5 seconds, or faster. This helps to improve visual attention span, which is your ‘bite size’ of visual information. Visual memory is extremely important for reading and is needed to build a sight word vocabulary. Visual sequential memory is particularly important for spelling.
- Organizing space - this section develops integration of skills, especially bilateral integration (coordinating the two sides of the body) and vision with movement. It is also aimed at developing laterality awareness and confidence which should help to overcome reversals of letters and numbers and confusion of the mirror image letters like b, d, p and q, when reading and writing.
- Eye movements - these activities help to develop good eye movement control which is essential for reading, handwriting and ball sports. Good eye movement control also helps to develop sustained attention. A component of these activities involves 'rapid automatic naming'. This skill links vision to oral language and is very important when learning to read.
- Brain Turning on your brain - these activities are designed to help develop better attention and concentration. Many of the tasks here also require integration of the different senses – vision, auditory (hearing) speech and movement - so that your child will learn to concentrate on several things at the same time. This also is a wonderful treatment for those with dyslexia and phonological delays.
- Student will move eyes and head to visually focus on ELA materials in horizontal, vertical and diagonal planes __ % of the time.
- Student will maintain visual attention on the teacher or other visuals ___% of the time.
- Student will be able to break words into syllables by rhythmically clapping to represent at least two syllables in a word __% of the time.
- Balance issues
- Blurred or double vision (child doesn’t know any different)
- Difficulty focusing and concentrating (looks like ADHD)
- Difficulty reading or writing or copying from board
- Dizziness or motion sensitivity
- Eye strain or fatigue (child doesn’t know difference as they have had this all their life)
- Headaches (many children have had headaches their entire lives and don’t know difference to complain) or overwhelmed easily needs breaks often
- Increased fall risk
- Increased fatigue
- poor central, peripheral or side vision
- Poor attention span
- poor balance
- Sensitivity to light
- eye poking
- reversals past age 6-7
- Difficulty transferring information from one page to next or board to paper
- poor coordination and difficulty with sports
- Vision therapy: This involves a series of structured activities and exercises designed to improve eye coordination, focusing abilities, eye tracking, and visual perception skills. Vision therapy may include activities such as motion processing, eye tracking exercises, convergence and accommodations exercises, focusing exercises, depth-perception training, and visual scanning tasks.
- Prism therapy: Prism lenses are used to alter the way light enters the eyes, which can help improve visual alignment and reduce symptoms such as double vision or eye strain. Prism therapy may be used to treat conditions such as strabismus (crossed eyes) or binocular vision dysfunction.
- Ocular motor exercises: These exercises focus on improving the coordination and movement of the eyes. They may involve activities such as tracking moving objects, following patterns with the eyes, or practicing smooth and accurate eye movements using techniques such as motion processing while utilizing various dynamic movement activities such as swings, balance beams, balance boards, and exercise balls.
- Visual perceptual training: This involves activities aimed at improving how the brain interprets and processes visual information. It may include tasks such as matching shapes or patterns, identifying objects in complex visual scenes, or discriminating between similar visual stimuli.
- Saccadic training: Saccades are rapid eye movements that allow us to shift our gaze from one point to another. Saccadic training exercises help improve the speed and accuracy of these eye movements, which can be beneficial for tasks such as reading or scanning a visual scene, or developing the ability to copy from board to paper.
- Visual memory exercises: These exercises aim to improve the ability to remember and recall visual information. They may involve tasks such as memorizing sequences of letters or numbers, recalling details from a visual scene, or matching objects based on memory.
- Piggy back program or other vision based HEPs: Piggyback is designed to develop and enhance the essential visual thinking skills needed for efficient learning and many other life skills. This program has a particular emphasis on the prerequisite visual information processing skills required for reading. It allows the development of these skills by encouraging your child to think for themselves through specific interactions between the child and their helper. By the continuous posing of questions from the helper the child is allowed to self discover.
- Adaptive techniques and equipment: Occupational therapists may recommend and teach individuals how to use adaptive equipment or techniques to help them perform attention, focus, reading and writing tasks more easily such as reading helpers that include highlighted lines, finger highlighters, inclined writing and reading boards, highlighted lined paper, seated attention helpers such as move and sit seat wedges, vibration to help central focus, weighted vests to help central attention, etc.
- Therapeutic activities & exercises: These are to address delays in vestibular-visual processing, praxis, reflex integration, muscle tone, laterality and directionality, visual tracking, saccades, visual motor, visual perceptual, fine motor, neck and core stability & strength that can all affect writing, reading and attention/focus.
- Environmental modifications: Occupational therapists may suggest modifications to the physical environment to help the child pay attention. Environmental modifications can also help them focus and take breaks as needed.
- Sensory integration therapy: This approach is used to help individuals with sensory processing disorders or sensory sensitivities learn to better process and respond to sensory input, such as touch, sound, or movement to decrease their stress level so they can pay attention, learn and be calm. No one learns when they are overwhelmed and the brain cannot retain what is learned if the brain or body is stressed.
Center of Development does a very comprehensive OT evaluation of all of the areas listed above and if your child has delays in these areas then medical based OT will be recommended.
Most medical based insurance plans require at least a 20% delay in several areas affecting daily life skills in order for us to bill your medical insurance for OT.
If your child does not have enough medical delays to bill insurance but you still want help in these areas then we will refer you to cash pay based Vision Therapy and OT performed by Kailey Mallard, OTR/L who is a Vision Therapist and OTR/L.
Our recommendation is to address the OT and Vision related issues 1st for best brain processing, these are the foundational skills needed 1st in the lower levels of the brain.
Power is a real focus of our therapies!
We recommend only doing reading and dyslexia tutoring programs after OT and Vision therapies are completed to make the brain & memory centers work most effectively and go quicker- and lighter on your pocket book for the best results in fastest time!
Our OTs work closely with Dr. Clopton regarding your child’s vision therapy but we require that you do the home exercises prescribed by Dr Clopton at least 20 min 5 nights a week for fastest results.
Please see Center of Vision and email [email protected] for more info on the cost of Piggyback home program and other home vision therapy programs that are used out of office.
In office OT/VT treatments are available see front desk for cash discounted pricing or contact [email protected] for an estimate of costs.
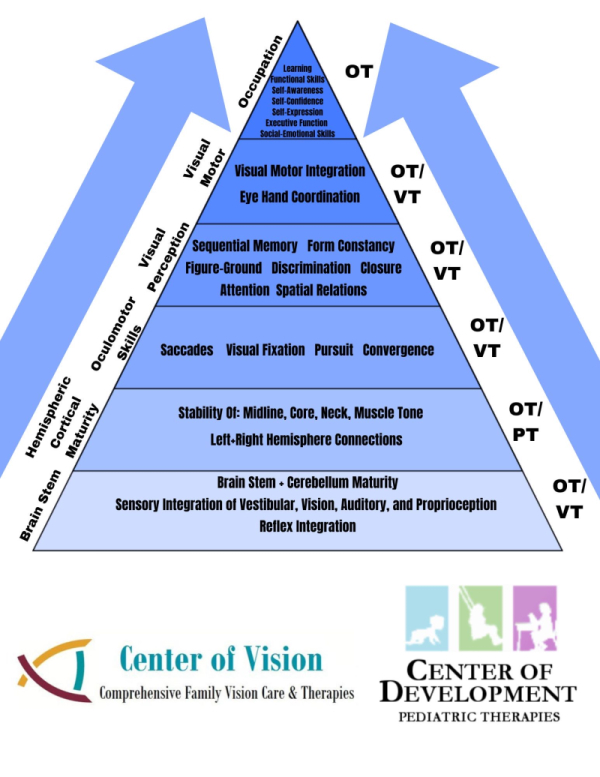
Areas that your COVD Eye Doctor will evaluate that other eye doctors, screenings or pediatrician do NOT have time for:
Oculomotor skills are those processes that move our eyes in order to take in information. Oculomotor control allows our eyes to move and retrieve visual input. These motor skills are crucial to retrieval and processing o visual information.
Visual Fixation- This is the ability to keep the eyes focused and steady without moving the eyes away from a specific target or visual stimuli. Fixation is necessary to maintain a steady gaze while the eye focuses on the most important part of the information that is being discerned. Visual fixation is a voluntary skill needed to focus vision on written material when reading.
Visual Saccades/Visual Scanning- Saccades are the ability to visually scan information. Saccades require the ability to fixate on information in the visual fields. Saccadic movement, or more commonly known as saccades, is the ability of the eyes to move in synchrony from point A to point B rapidly WITHOUT deviating from the path.
Eye Smooth pursuits/Visual Tracking- allow visual tracking of a moving item. This visual skill is needed in tasks where the eyes follow a moving visual target such as a ball, or a teacher who is moving around the classroom. The eye’s ability to move and visually track information is both an automatic (reflexive) response and a voluntary action. Tracking allows us to follow a moving object as it moves across our field of vision. Visual tracking also includes the ability to move the eyes in various directions!
Visual Convergence- Convergence and divergence is an eye teaming skill. This controlled use enables both eyes to focus on a single object, with the brain combining the two visual images into one, and with regards to the depth of the object in relation to the eyes is otherwise known as binocular fusion. Convergence insufficiency hinders the child’s ability to move their eyes in synchronized, coordinated, and smooth movements from a far point to a near point or near point to far point.
Why Piggyback home program helps reading!
Dr Clopton, Heidi Clopton OTR/L & Kailey Mallard OTR/L are certified providers for Piggyback! This is an Australian based developmental home program that is excellent to address all areas of development to build a BRAIN and BODY that are READY to LEARN!
DEVELOPMENTAL VISION THERAPY COMPUTER-ASSISTED Home Treatment
Piggyback’ is designed to develop and enhance the essential “visual thinking skills” needed for efficient learning and many other “life skills”. ‘Piggyback’ has a particular emphasis on the pre-requisite visual information processing skills required for reading like subcortical processing like reflex integration, then cortical processing skills for R & L hemispheric development, all the way up to phonological skills.
It is called Piggyback because it is designed to help give the FOUNDATION for reading to develop- once they do Piggyback then they often only need school or tutoring based reading help to overcome their reading delays or even “dyslexia”.
It is creating the neural pathways that are not developed for reading.
‘Piggyback’ is not a reading instruction program. Specific reading instruction should be undertaken by teachers who are trained in this field. ‘Piggyback’ is designed to improve visual thinking skills and it therefore is expected that there will be a greater ability to learn, focus, improved visual attention, and reading after completing the program.
‘Piggyback’ is divided into nine levels. Each succeeding level builds on the previous level so it is extremely important that every activity is completed before moving on. Unless otherwise instructed by us level 1 is completed before proceeding to level 2 and in turn level 2 is completed before starting level 3 etc.
It may take between 2 and 6 weeks to complete each level of the ‘Piggyback’ program. By spending 20 to 30 minutes, 5 days per week, maximum benefits should be obtained from this program.
Each activity is designed so that when first attempted it can be completed, but with some difficulty and a great deal of thinking.
With repeated practice however, efficiency improves, much less thinking is required and the task becomes automatic.
Therefore, repeated practice of each activity is absolutely essential to develop skills required to achieve the goals within each task. Once each goal has been reached, the skills developed should not be lost and usually will not require further practice to be maintained a permanent neural pathway has been created.
We would like to see you in-office every 4 to 6 weeks to ensure activities are understood and completed, and to answer any arising questions.
The ‘Piggyback’ program costs are NOT COVERED by insurance as insurance does not cover any type of home programming.
We do not do in office vision therapy with a vision therapist anymore due to the low $12 reimbursement we received and cannot afford to keep a vision therapist employed at this rate.
‘Piggyback’ is only sold under copyright, by prescription of Dr Clopton and cannot be purchased “over-the-counter”.
‘Piggyback’ is divided into five sections. Each section develops specific skills. These sections are:
Center of Vision and DR Clopton have a very high success rate when families do Piggyback every day and get through all the levels!
Other online VT- OT- READING RESOURCES & Exercise Home Program links:
TN Disability Path Finder look up reading specialists and Dyslexia specialists in your area.
https://www.facebook.com/share/yHZyVpGz5SjoH4ut?mibextid=WC7FNe
Excellent resource for Dyslexia treatment:
Reading 360: Tennessee Literacy program
Learning: online education website Online public school in TN
Lots of FREE resources
Free:
phonogram-sounds-app
Free reading games
Other free resources
Dyslexia Advantage
Great Videos for Home program exercises:
Reflex Integration
Fear Paralysis Tapping
Fear Paralysis Tapping
Moro integration
Harder version later
Harder version later
Figure Eight abc drawing
Infinity Walk
infinity to a beat
Center of Development bdpq, figure eight, etc. exercises- R/LBrainExercises
Weighted cross crawl
Weighted cross crawl
Body Codes
Visual Tracking Exercises with ball hung from ceiling fun
Easy at home visual tracking & eye hand coordination
Easy at home visual tracking & eye hand coordination
VOR CHART Vestibular swinging & visual eye hand exercises
VOR CHART Vestibular swinging & visual eye hand exercises
Science of Reading" Is Important, But Can We Please Talk About Occupational Therapy's Role In Interventions?
The "science of reading" is a trending topic nationwide, as school divisions reevaluate what they thought they knew about reading and how they've instructed students. However, being taught the necessary skills to read and write involves more than teaching children encoding and decoding. It involves learning how to hold a book and a pencil, tracking words on a page or screen, learning what strategies to use when fatigue or frustration overcome them, learning how to best advocate when they are struggling, identifying assistive technology to help them and teaching them how to use the assistive technology, and identifying and providing the specially-designed instruction needed to teach students this other side of reading and writing, and how to practice and perfect it.
Experts in the field of occupational therapy have for years advocated for occupational therapists being included in reading and writing intervention teams.
In an April 26, 2016, article published in “Journal of Occupational Therapy”, Dr. Gloria Frolek Clark emphasized the role of the occupational therapist in working with reading and writing teams: “Nationally, student proficiency in reading and writing is very low and requires ongoing focus from state and local agencies. With almost 25% of occupational therapists working in early intervention and school settings (AOTA, 2015), their role of facilitating literacy (e.g., reading, writing, speaking and listening) is critical. Occupational therapy practitioners support the development and growth of literacy at the system, home or school, and individual levels.”
A year later, April 27, 2017, in the article “OT and PT Support for Literacy in Schools”, Jean Polichino emphasized the importance of occupational therapy and physical therapy being included in reading and writing interventions. "Stamina" is one of the areas she suggests addressing: “Interventions to Promote Access and Reduce Barriers: Development of physical stamina and balance, if these are interfering with the child's ability to make progress in literacy areas."
January 15, 2019, “The Open Journal of Occupational Therapy” published the article titled “The Role of Occupational Therapy in Functional Literacy”, by experts in the field, Dr. Lenin C. Grajo and Dr. Sharon A. Gutman. In the article, Grajo and Gutman focus on functional literacy and the occupational therapist’s role in providing therapy, and they cite U.S. Department of Health and Human Services “Healthy People 2030” initiative, which focuses on functional literacy: “One of the foundational principles of Healthy People 2030, a U.S. Department of Health and Human Services (2017) initiative, is the achievement of health and well-being through the elimination of health disparities, the achievement of health equity, and the attainment of health literacy. Occupational therapists can have a critical role in eliminating health disparities by not only facilitating clients’ health literacy but also addressing functional literacy. As occupational therapists, we have traditionally supported clients in literacy development by addressing prerequisite skills, such as visual-motor and perceptual skills, fine motor skills, cognitive and executive function skills, and sensory processing skills. Given the impact of literacy challenges on health, well-being, and adaptation, however, our roles cannot end with supporting prerequisite skill development alone. A holistic approach to functional literacy must promote literacy from the perspective of occupational participation and the enhancement of resiliency in the face of literacy challenges.
One example of this practice is the Occupation and Participation Approach to Reading Intervention (Grajo & Candler, 2016), in which occupational therapists work conjointly with clients to develop the literacy strategies of adaptation, compensation, and remediation. Examples of adaptation could include strategies to reduce the amount of screen/page words to enhance visual attention and organization, magnifiers to increase readability, replacing or coding words with pictographs and photos that enhance learning and comprehension, using tactile aids and colored highlighting to increase visual attention to important details, and teaching clients to take structured breaks to reduce cognitive overload.
Compensation could include such methods as using mnemonics to assist memory and voice activated technology to interpret unfamiliar words and obtain needed information.
Remediation would involve the practice of real-life occupations requiring functional literacy skills, such as check writing, bill paying, ATM machine use, transportation schedule interpretation, meal preparation using package directions, medication label interpretation, and written job application submission. In these activities, occupational therapists must continuously ask, “What strategies and tools does the client use to overcome literacy challenges?” “Are the client’s strategies and tools effective?” “How can I facilitate the development of new tools and strategies that may be more effective?”
In a separate “Occupational Therapy for Literacy Development” presentation hosted by Colorado Department of Education, Dr. Lenin Grajo further emphasized the importance of occupational therapists being a part of literacy intervention teams. In the powerpoint slides for the presentation, he includes some of the following examples of goals related to vision therapy:
April 13, 2023, the journal “Applied Neuropsychology: Child” published the article “Effects of the Visual Praxis-Based Occupational Therapy Education Program on different kinds of reading skills: Single-blind randomized follow-up study”. The results of the study provide additional proof of visual-based occupational therapy helping students with reading:
When we talk about reading and writing, we must look at the complete picture and we must include professionals from a wide range of arenas—not just the English teacher—in reading and writing interventions.
As occupational therapists, it is imperative that we rule out vision problems before treating handwriting or delays in visual motor integration, to ensure the best possible trajectory of development and success for the child.
A developmental optometrist (COVD.org to find one near you) will complete a full evaluation and determine the need for corrective lenses, vision therapy or a home program to address vision concerns.
Common symptoms of vision impairment include:
Per AOTA-
Neuro-visual therapy:
Neuro-visual therapy is a type of therapy that focuses on addressing visual processing issues that may affect a person's overall well-being and functioning. It involves exercises and techniques aimed at improving the coordination between the eyes and the brain, as well as enhancing visual perception and processing abilities.
This therapy is often used to treat conditions such as convergence insufficiency, amblyopia (lazy eye), strabismus (crossed eyes), binocular vision dysfunction, and other visual problems that can impact daily activities, such as reading, driving, and sports performance. Neuro-visual therapy may include activities such as eye exercises, vision training, visual scanning tasks, hand-eye coordination exercises, home programs, and specialized computer-based programs designed to improve visual skills.
It's typically administered by optometrists or vision therapists who are specially trained in assessing and treating visual processing disorders. The goal of neuro-visual therapy is to help individuals improve their visual abilities, enhance their quality of life, and achieve better overall functioning.
Common neurovisual interventions include various exercises and techniques aimed at improving visual processing and function. Some of these interventions may include:
For more information please contact [email protected].
These interventions are typically tailored to the specific needs and goals of each individual and are often administered under the guidance of a trained optometrist or vision therapist. The duration and frequency of neuro-visual therapy sessions may vary depending on the severity of the visual issues and the individual's progress.
Occupational therapy:
Occupation refers to activities that support the health, well-being, and development of an individual (American Occupational Therapy Association, 2014). For children and youth, occupations are activities that enable them to learn and develop life skills (e.g., preschool and school activities), be creative and/ or derive enjoyment (e.g., play), and thrive (e.g., self-care and relationships).
Occupational therapy practitioners work with children, youth, youth families, caregivers, and teachers to promote active participation in activities or occupations that are meaningful to them.
Working with children of all ages and abilities through the habilitation and rehabilitation process.
They collaborate with parents/caregivers and other professionals to identify and meet the needs of children experiencing delays or challenges in development, and collaborate to identify and modify or compensate for barriers that interfere with, restrict, or inhibit functional performance.
The main goal of occupational therapy is to enable individuals to participate in activities that are important to them, despite any limitations they may have.
Some common interventions used in occupational therapy include:
Copyright © 2015 by the American Occupational Therapy Association. This material may be copied and distributed for personal or educational uses without written consent.
Contact me for more info
Heidi Clopton OTR/L
Pediatric Occupational Therapist
Therapy Director & Owner
[email protected]
Center of Development
Pediatric Therapies
www.developmentaldelay.net
Site empowered by
WebOnTheFly